

A stroke or cardiovascular accident, sometimes known as a “brain attack”, is caused by an interruption of nutrients and oxygen to the brain because of a blockage. This can be caused by a blood clot, an atherosclerotic plaque, trauma, brain surgery, or rupture of a vessel or aneurysm, among others. There are many causes of stokes but it is defined by a mechanical blockage that interrupts the flow of blood in the vessels that bring new nutrients to brain tissue.

The flow of blood is stopped and/or the blood vessel ruptures causing further interruption of blood flow. The tissue that is beyond the blockage will starve and die.
TYPES OF STROKES
Ischemic (lack of blood supply) strokes

These are the most common type of stroke. They are caused by a clot, either atherosclerotic or blood, lodged in a tiny cerebral artery which results in death of brain tissue.

This kind of ischemic event is the same thing that happens during a heart attack. During a stroke the clot simply lodges in a different place, your brain instead of your heart, and that’s why the root cause of strokes for the most part, is considered to be heart disease.
Lacuner Stroke

This type of stroke constitutes about 25% of ischemic strokes. Deep penetrating arteries in the brain become occluded with small clots and cause a lacune (Latin for Lake) of “empty fluid” (whatever that means) in the region. Lacunar strokes are primarily the result of small vessel disease.
Small vessel disease

The arteries that deliver fresh oxygen throughout your body with every beat of your heart eventually become smaller and smaller in the peripheral circulation or in the deep tissues of your body. These tiny arteries or arterioles,join in a web at the very end of your tissue with similarly tiny veins or venules, and give up their oxygen. They then continue as veins which in turn become larger and larger until they return all of the oxygen- depleted blood back to the heart to get some more oxygen.
Small vessel disease occurs in the region where the vessels become reduced in size. And there’s considered two kinds of small vessel disease; peripheral arterial disease, in blood vessels supplying nutrients to the tissues, and peripheral venous disease, in blood vessels returning to the heart for a refill. People with small vessel disease have trouble in these distant regions of oxygen exchange so vital to feeding cells. Lacunar strokes can be caused by weakened vessel walls from elevated blood pressure, by malformations, or can be occluded by a blood clots or atherosclerotic clots.

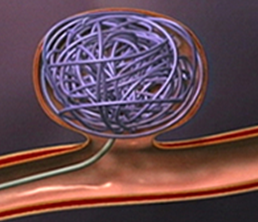
Arterial-venous (AV) malformations
This is a congenital disease of the brain that can mimic stroke-like symptoms. The arterial-venous capillary bed described above is mal-formed in the fetus. The bigger arteries and veins connect without having the normal tiny connections, making this area vulnerable to pressure and rupture.

These vessels bypass what capillary bed there is and create a nidus or nest; a tangle of blood vessels that are fragile and prone to breakage, and can cause seizures, headaches and bleeds. An abnormal circulation develops creating a rapid blood flow that makes a “whooshing” sound that patients can actually hear in their heads. This understandably can disrupt sleep and cause tremendous anxiety for the patient.

This is a young person’s disease for the most part, and often occurs in teenagers and young adults. The treatment is usually embolization, which means the vessels leading to the AVM are “embolized” or blocked off through a surgical procedure, so that blood will no longer take that route thus decreasing the pressure on the nest of blood vessels.
Embolization

Embolization
Smoking
Smoking

Smoking is especially detrimental because nicotine causes vaso-constriction (tightening) and spasm in these already small arterioles, and carbon monoxide, a product of smoking, decreases the amount of oxygen available to the blood. So the heart has to work harder and beat faster which elevates blood pressure even more, putting additional strain in these little vessels. Round and round and round we go.
Transient Ischemic Attacks or TIAs. (Mini Strokes)
TIAs are little strokes just practicing for the big one. They are a warning sign not to be ignored. These are essentially strokes of short duration (not more that 24 hours) and they are usually ischemic events that cause neurological symptoms of varying duration, lasting seconds to hours. Usually these symptoms can present as difficulty speaking, visual problems, limb weakness, or numbness and tingling. Occasionally patients feel dizzy or uncoordinated, or just have a vague feeling that something’s wrong. TIAs are warning shots across the bow-so heed them well.

BLOOD CLOTS
Atrial Fibrillation
Atrial Fibrillation
Blood clots can be caused by atrial fibrillation,an irregular electrical pattern in the heart which causes the heart to beat in a weak, less coordinated way. The atrial chambers flutter or fire ineffectively,causing the ventricles to contract irregularly, and making the flow of blood from the heart less vigorous.

Normal rhythm (above)-The atria contacting (small spike) followed by the ventricles contracting (big spike). Notice how they work in nice sharp sequence.

Atrial Fibrillation- the red arrow points to multiple ineffective contractions of the atria that do not cause the big ventricular contraction. The purple arrow indicates normal rhythm.
When the heart is not able to fully expel blood in a heartbeat because of this weakened ineffective action, some blood is left behind in the heart chambers and the reduced flow of that blood allows clots to form. Doctors will check for this as a cause for your stroke by doing an electrocardiogram which will show the irregular beat.
Atrial fibrillation is often asymptomatic and is not in itself generally life-threatening, but it may result in palpitations, fainting, chest pain, or congestive heart failure. People with AF usually have a significantly increased risk of stroke (up to 7 times that of the general population).* Wikipedia

If atrial fibrillation is severe your doctor may put you on digitalis, a drug derived from the foxglove plant, that slows down the rate that your atria beat and improves electrical conductivity to the ventricles.
Foxglove or Digitalis

Most stroke patients are prescribed anti-clotting agents,or blood thinners, to prevent clot formation. Those with atrial fibrillation are often given Warfarin. Warfarin in stronger amounts is also known as rat poison, and works by causing the rat to bleed to death. Human doses are of course safer.
As with any anti-coagulant, watch for signs of bleeding like excessive bruising or blood in your stool.

You may be prescribed baby aspirin daily, Plavix or Aggronox which has aspirin in it. Studies show that Aggronox has the best track record for secondary prevention of stroke but it can cause severe headaches. Your doctor will take blood tests periodically to see that you have adequate anticoagulation levels in your blood.
Carotid Patency
Carotid Patency
Clots can also be caused by atherosclerotic plaque or fatty build up in your arteries caused by too high levels of cholesterol. The two main carotid arteries that supply blood flow to the brain can become blocked by plaque causing the blood flow through them to be turbulent and slow down, making blood clot formation more likely.* see treatments below

Hemorrhagic strokes

The picture above shows a large dark area where blood has leaked from an artery.
Hemorrhagic strokes are caused by the rupture of a blood vessel in the brain either by the weakening of the vessel wall because of a lodged particle in the vessel or because of a genetic predisposition or malformations that causes the blood vessel to rupture under pressure. These ruptures are called Berry Aneurysms because the aneurysm first appears as a sac-like shape before it ruptures.


The treatment for Berry Aneurysm, if caught in time, is surgical tying-off of the weakened area.

Research has also shown that strokes can occur from sudden movement, intense anger or emotion. Golfers have been known to get a small tear in their carotid artery after swinging at a ball. In older folks, jumping up too fast to answer the doorbell,or being startled by the ring of the phone can be causative. Do we need more evidence for keeping our stress level down?
Early Treatment and Diagnosis
Sometimes after the initial event the stroke extends itself because the original damage to the arterial cell wall near the clot becomes weakened further with time and ruptures again. This is what happened to me the second day I was in the hospital. This is another reason not to second guess your diagnosis (mea culpa) and get yourself to the emergency room as soon as is humanely possible. Having TPA might well stop or limit the extent of damage.
TRY TO HAVE SOMEONE NOTE THE EXACT TIME OF SYMPTOM ONSET BECAUSE TPA CAN ONLY BE GIVEN IN A 3-HOUR WINDOW.
TRY TO HAVE SOMEONE NOTE THE EXACT TIME OF SYMPTOM ONSET BECAUSE TPA CAN ONLY BE GIVEN IN A 3-HOUR WINDOW.

As soon as possible after you have been diagnosed with a stroke, the doctor will assess if you are eligible for Tissue Plasminogen Activator (TPA), or the clot-busting drug.(Time is crucial here as TPA can’t be given outside of a three hour window that starts with your first symptoms, for fear of even greater bleeding.)
That’s why it’s so important to get immediate attention when symptoms start, to open up this blockage to return blood flow to the dying tissue beyond the clot. The doctors assess the amount and cause of bleeding by using a CT scan. This early evaluation is important because if the stroke were caused by a ruptured aneurysm instead of a blood clot for example, giving TPA or further anticoagulant your brain and causing more bleeding, would be disastrous.
CT Scans or X-ray Computed Axial Tomography

{kind=link}
You are likely to be given a CT Scan fairly soon after arrival in the emergency room. This computer assisted x-ray creates a 3D image from many layers of 2D x-rays and is most helpful in pin-pointing the extent of damage or bleeding so that treatment methods can be decided. It gives the doctor eyes and helps to avoid costly errors like giving a bleeding stroke patient anti-coagulant,or to identify a Berry Aneurysm that might require surgical intervention. This procedure has a fairly high radiation risk, but must be balanced with the risk of incorrect treatment.
A Carotid Doppler test is often done post-stroke to see if blood flow in the carotid vessels is normal. A Doppler works by bouncing sound waves off tissue to assess patency of the artery.

If the blockage is severe the doctors may advise surgically clearing out of the vessels a procedure known as carotid endaderectomy.


A coil or stent may also be inserted to correct poorly shaped arteries and maintain patency. These stents are also use to maintain flow within the heart when blood flow is deemed inadequate.

{kind=link}
In surgery a balloon might also be used to clear plaque and in a small number of patients a small filter or trap might used or permanently installed in the carotid arteries to catch further blood clots or debris if it is deemed necessary.

MRI or Magnetic Resonance Imagery

This is generally not used as an emergency test, but given further along in the hospital stay. It offers excellent contrast, sometimes with the use of intravenous contrast agents, so the radiologist can clearly see the soft tissues of the brain.


The American Heart Association (see link below on list of Medical Associations)) describes claw feet in an excerpt from “A Toe Curling Experience”, Stroke Connection Magazine, March/April 2004 (Science Update @009):

 Because toe muscles are typically not very strong, the contracting muscle overpowers the muscles in the toe. This tightens the tendons, causing the joints of the smaller toes to buckle or curl in an unnatural way. Claw toe most often strikes the stroke-side foot. Painful blisters may develop on the affected toes where their tips dig into the shoe. Added pressure from the imbalance may also cause calluses or corns to form on the ball of the foot. Claw toe also affects patients with joint diseases such as rheumatoid arthritis, cerebral palsy, nerve damage due to poor circulation, as with diabetes, and those confined to bed for a long time.
Because toe muscles are typically not very strong, the contracting muscle overpowers the muscles in the toe. This tightens the tendons, causing the joints of the smaller toes to buckle or curl in an unnatural way. Claw toe most often strikes the stroke-side foot. Painful blisters may develop on the affected toes where their tips dig into the shoe. Added pressure from the imbalance may also cause calluses or corns to form on the ball of the foot. Claw toe also affects patients with joint diseases such as rheumatoid arthritis, cerebral palsy, nerve damage due to poor circulation, as with diabetes, and those confined to bed for a long time.
Follow your doctor's instructions and use a splint or athletic tape to reposition the toes. Avoid shoes with heels over two inches. Wear soft shoes with plenty of room for the toes. Give your toes a workout by using them to pick up small objects such as marbles or a crumpled towel.
Looks kind of like a frog doesn’t it?
The MRI is a noisy, tight fit and may be very anxiety causing if you have claustrophobia. It’s important to let the technician know that you’re a claustrophobic, and they will give you a short-acting sedative. It’s better to go into the procedure aware of the drawbacks so you are ready, because it’s very important not to move. You are given an emergency button to hold onto if you get anxious. Once you’ve been moved into place via a sliding bed, you are surrounded by a large circular machine that is very close to your head and which emits loud hammering noises intermittently. I’ve had several of these scans and they make me extremely uncomfortable, but I can get through it. I close my eyes and try not to think about how tight the space is and focus my mind on something else, but I don’t enjoy it. I have not yet needed a sedative. Sometimes they give you an intravenous infusion of contrasting dye. You are very aware when it’s being infused because it tastes pretty foul .
Discovery Heath gives a great explanation of how an MRI works if you are interested in knowing a little more detail.
http://health.howstuffworks.com/medicine/tests-treatment/mri.htm

Most Canadians who suffer a stroke wait too long before they seek medical treatment. And when they finally show up at a hospital, their cases aren’t always dealt with promptly. Those are the main conclusions of a study by the Canadian Stroke Network, which is composed of university and hospital researchers.
Oct 3/11
Strokes are a race against time:
http://www.theglobeandmail.com/life/health/new-health/paul-taylor/strokes-are-a-race-against-time-study/article2064003/

Oct 5/2011
Carotid artery occlusion

http://www.angiologist.com/carotid-artery-occlusion/
Medical treatment
Claw Toes
Curling of the toes on the affected side can get worse with time for those whose limbs are affected by stroke and a well-built shoe can help keep them flatter as well as assist in maintaining a gait that does not contribute to toe curling. This curling of the toes is called a “claw foot”.
Excerpted from "A Toe-Curling Experience," Stroke Connection Magazine, March/April 2004 (Science update August 2009)
About six months after Katherine Ware had a stroke in 1996, she noticed that her small toes had begun to curl beneath her left foot. Wearing shoes became problematic and walking was painful. Her stroke physician referred her to a podiatrist, who identified her malady — a condition called “claw toe.”
Claw Toe
Claw toe, and a similar condition called “hammertoe,” are caused by an imbalance of muscles in the feet and toes. Brain injury during a stroke leaves survivors prone to neuromuscular imbalances. With claw toe, muscles in the foot over-contract due to a neurological abnormality.
Claw toe, and a similar condition called “hammertoe,” are caused by an imbalance of muscles in the feet and toes. Brain injury during a stroke leaves survivors prone to neuromuscular imbalances. With claw toe, muscles in the foot over-contract due to a neurological abnormality.
Claw toe and hammertoe are very similar conditions, differing in the muscles affected — flexor digitorum brevis and flexor digitorum longus, respectively. For this reason, the terms “claw toe” and “hammertoe” are often used interchangeably.
Claw toe is classified in two ways — “flexible” or “rigid” — based on the severity and progression of the condition.
Flexible Claw Toe
“Flexible claw toe” describes the earlier stages in which, as the name suggests, the toes are still flexible at the joint. The American Academy of Orthopaedic Surgeons (AAOS), in conjunction with the American Orthopaedic Foot and Ankle Society, offers these suggestions for helping to correct the imbalance of flexible claw toe:
“Flexible claw toe” describes the earlier stages in which, as the name suggests, the toes are still flexible at the joint. The American Academy of Orthopaedic Surgeons (AAOS), in conjunction with the American Orthopaedic Foot and Ankle Society, offers these suggestions for helping to correct the imbalance of flexible claw toe:
Rigid Claw Toe
“Rigid claw toe” designates the later stages in which the toes are fixed in this unnatural position. As the tendons tighten and the deformity becomes fixed, fewer options are available. Non-surgical treatments are confined more to pain-management than to correcting the condition. To minimize discomfort for rigid claw toe, the AAOS recommends trying specialized shoes “that have an extra 3/8” depth in the toe box” or asking a “shoe repair shop to stretch a small pocket in the toe box to accommodate [the toes].”
“Rigid claw toe” designates the later stages in which the toes are fixed in this unnatural position. As the tendons tighten and the deformity becomes fixed, fewer options are available. Non-surgical treatments are confined more to pain-management than to correcting the condition. To minimize discomfort for rigid claw toe, the AAOS recommends trying specialized shoes “that have an extra 3/8” depth in the toe box” or asking a “shoe repair shop to stretch a small pocket in the toe box to accommodate [the toes].”
Katherine Ware, a stroke survivor, recommends a different option: surgery. “I’d be on a cane if it weren’t for the surgery,” she said. The procedure involved cutting the tightened tendons. Other possible procedures include lengthening or repositioning tendons, or shortening the bone of the toe. Inserting a steel pin into the toe often corrects the problem.
As with all surgeries, infection is a risk, and swelling and pain are common in the following weeks. Ware says her surgery was “easy” with a “quick recovery.” Although typically no tests are needed to identify claw toe, an X-ray will most likely be required if surgery is considered.
Lillian Schwartz, a stroke survivor in Boca Raton, Fla., uses foam toe separators. Available at beauty supply stores for just a few cents, the separators are used by beauticians when giving pedicures. Schwartz recommends using two separators (one on top of the other) if your toes are long. James Pribish, a stroke survivor from New Castle, Del., uses a pair of gel insoles with tiny magnets embedded in them, which he says have greatly reduced the curling.
Botulinim toxin (Botox®) as Treatment
Botulinim toxin (Botox®), a complex protein byproduct of the bacterium famous for contaminating canned goods and homemade preserves, is another treatment option. Botulinim toxin has the highest toxicity of all known substances, so it seems odd that it has found its way to the forefront of medical technology. But the toxin, injected in tiny amounts at the site of the over-contracted muscle, has given relief.
Botulinim toxin (Botox®), a complex protein byproduct of the bacterium famous for contaminating canned goods and homemade preserves, is another treatment option. Botulinim toxin has the highest toxicity of all known substances, so it seems odd that it has found its way to the forefront of medical technology. But the toxin, injected in tiny amounts at the site of the over-contracted muscle, has given relief.
For a muscle to contract, it must receive a chemical signal (neurotransmitter) from a nerve ending. Botulinim toxin injections block the nerve endings. This keeps the neurotransmitters from reaching the nerve and signaling the muscle to contract. The effects aren’t usually noticed for five to 10 days and last only three to four months.
Not much is widely know about claw toe, but you can get help for this painful condition. If your doctor doesn’t know much about it, seek more help, and ask more questions.
